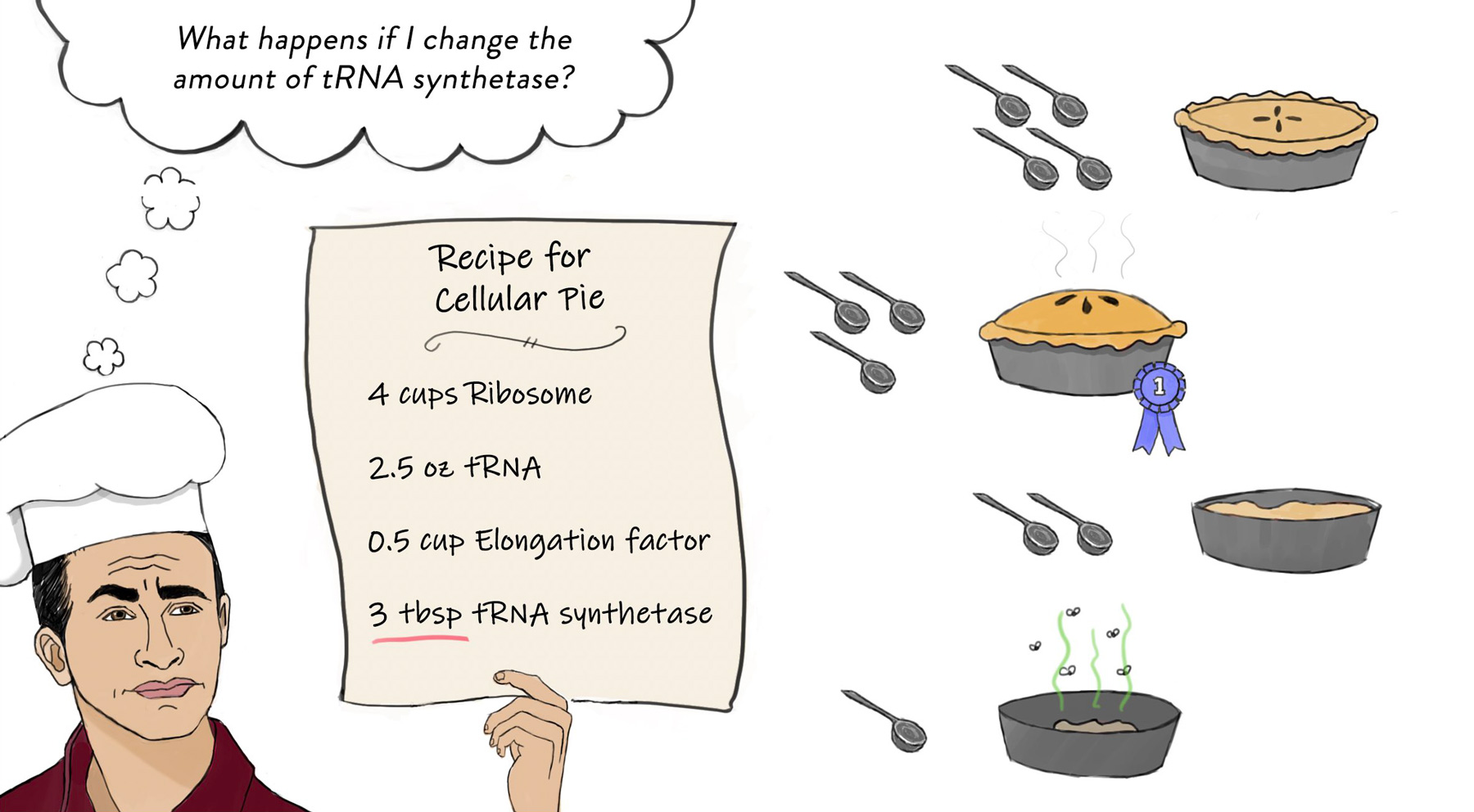
Researchers discover new rules governing bacterial gene expression that overturn fundamental assumptions about basic biological pathways.
Raleigh McElvery
August 26, 2020
On the evolutionary tree, humans diverged from yeast roughly one billion years ago. By comparison, two seemingly similar species of bacteria, Escherichia coli and Bacillus subtilis, have been evolving apart for roughly twice as long. In other words: walking, talking bipeds are closer on the tree of life to single-celled fungus than these two bacteria are to one another. In fact, it’s becoming increasingly clear that what is true of one bacterial type may not be true of another — even when it comes down to life’s most basic biological pathways.
E. coli has served as a model organism in scientific research for over a century, and helped researchers parse many fundamental processes, including gene expression. In these bacteria, as one molecular machine, the RNA polymerase, moves along the DNA transcribing it into RNA, it is followed in close pursuit by a second molecular machine, the ribosome, which translates the RNA into proteins. This “coupled” transcription-translation helps monitor and tune RNA output, and is considered a hallmark of bacteria.
However, an interdisciplinary team of biologists and physicists recently showed that the B. subtilis bacterium employs a different set of rules. Rather than working in tandem with the ribosome, the polymerase in B. subtilis speeds ahead. This system of “runaway” transcription creates alternative rules for RNA quality control, and provides insights into the sheer diversity of bacterial species.
“Generations of researchers, including myself, were taught that coupled transcription-translation is fundamental to bacterial gene expression,” says Gene-Wei Li, an associate professor of biology and senior author of the study. “But our very precise, quantitative measurements have overturned that long-held view, and this study could be just the tip of the iceberg.”
Grace Johnson, a graduate student in the Department of Biology, and Jean-Benoît Lalanne, a graduate student in the Department of Physics, are the lead authors on the paper, which appeared in Nature on Aug. 26.
A curious clue
In 2018, Lalanne developed an experimental technique to measure the boundaries of RNA transcripts. When DNA is transcribed into RNA, the resulting transcripts are generally longer than the DNA coding sequence because they also have to include an extra bit at the end to signal the polymerase to stop. In B. subtilis, Lalanne noticed there simply wasn’t enough space between the ends of the coding sequences and the ends of the RNA transcripts — the extra code was too short for both the polymerase and the ribosome to fit at the same time. In this bacterium, coupled transcription-translation didn’t seem possible.
“It was a pretty weird observation,” Lalanne recalls. “It just didn’t square up with the accepted dogma.”
To delve further into these puzzling observations, Johnson measured the speeds of the RNA polymerase and ribosome in B. subtilis. She was surprised to find that they were moving at very different rates: the polymerase was going roughly twice as fast as the ribosome.
During coupled transcription-translation in E. coli, the ribosome is so closely associated with the RNA polymerase that it can control when transcription terminates. If the RNA encodes a “premature” signal for the polymerase to stop transcribing, the nearby ribosome can mask it and spur the polymerase on. However, if something goes awry and the ribosome is halted too far behind the polymerase, a protein called Rho can intervene to terminate transcription at these premature sites, halting the production of these presumably non-functional transcripts.
However, in B. subtilis, the ribosome is always too far behind the polymerase to exert its masking effect. Instead, Johnson found that Rho recognizes signals encoded in the RNA itself. This allows Rho to prevent production of select RNAs while ensuring it doesn’t suppress all RNAs. However, these specific signals also mean Rho likely has a more limited role in B. subtilis than it does in E. coli.
A family trait
To gauge how common runaway transcription is, Lalanne created algorithms that sifted through genomes from over 1,000 bacterial species to identify the ends of transcripts. In many cases, there was not enough space at the end of the transcripts for both the RNA polymerase and the ribosome to fit, indicating that more than 200 additional bacteria also rely on runaway transcription.
“It was striking to see just how widespread this phenomenon is,” Li says. “It raises the question: How much do we really know about these model organisms we’ve been studying for so many years?”
Carol Gross, a professor in the Department of Microbiology and Immunology at University of California San Francisco who was not involved with the study, refers to the work as a “tour de force.”
“Gene-Wei Li and colleagues show transcription-translation coupling, thought to be a foundational feature of bacterial gene regulation, is not universal,” she says. “Instead, runaway transcription leads to a host of alternative regulatory strategies, thereby opening a new frontier in our study of bacterial strategies to thrive in varied environments.”
As researchers widen their experimental radius to include more types of bacteria, they are learning more about the basic biological processes underlying these microorganisms — with implications for those that take up residence in the human body, from helpful gut microbes to noxious pathogens.
“We’re beginning to realize that bacteria can have distinct ways of regulating gene expression and responding to environmental stress,” Johnson says. “It just shows how much interesting biology is left to uncover as we study increasingly diverse bacteria.”
Citation:
“Functionally uncoupled transcription–translation in Bacillus subtilis”
Nature, online August 26, 2020, DOI: 10.1038/s41586-020-2638-5
Grace E. Johnson, Jean-Benoît Lalanne, Michelle L. Peters, and Gene-Wei Li